
Non specific lower back pain - Understand it better!

Non specific lower back pain (NSLBP) is the most common MSK problem world-wide. It is also an often-misunderstood problem! This will help to de mystify what NSLBP is & is not & hopefully provide positive information to pass on to those suffering with NSLBP
What is it? “pathoanatomical cause of the pain cannot be determined” - Maher
“For nearly all people presenting with low back pain, the SPECIFIC nociceptive source cannot be identified” - - Foster
“Presumed MSK origin of LBP. No tests available to specify SOURCE reliably” – Bardin
https://pubmed.ncbi.nlm.nih.gov/27745712/
https://pubmed.ncbi.nlm.nih.gov/28359011/
So NSLBP is actually a pretty broad label, even though it is one of exclusion NSLBP could be muscular, tendinous, ligamentous, joint related or discogenic & these cannot differentiated via clinical testing It could also be contributed to by many things across the BPS spectrum
Its not something specific! 1% is serious pathology 5-10% is specific, Radicular (nerve root), Radiculopathy (Nerve function) & Stenosis (neurogenic claudication The rest is non specific as earlier described (90-95%)
https://pubmed.ncbi.nlm.nih.gov/33579691/
Imaging Early imaging to reduce uncertainty can be common in healthcare This has been now seen as something that should be reduced without a good clinical reason to do so
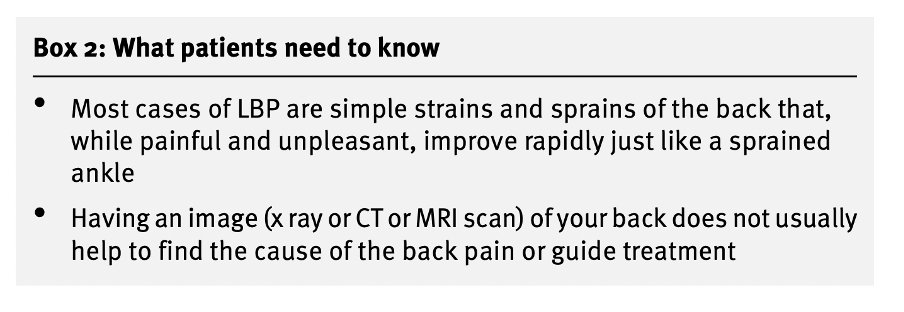
It seems to! A process of care that that included Nonconcordant diagnostic imaging such as X ray or MRI increased risk of acute LBP transitioning to chronic LBP
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2776518
So the news is good? Well yes, I think so “good prognosis & low risk of serious disease” I describe it as “not medically serious, but seriously painful & disruptive to our lives” It’s important not to invalidate the problem
Is Non specific a “bad term”? "‘Episode of back pain’, ‘lumbar sprain’ and ‘non-specific LBP’ reduced need for imaging, surgery and second opinion compared to ‘arthritis’, ‘degeneration’ and ‘disc bulge’"
https://onlinelibrary.wiley.com/doi/full/10.1002/ejp.1981
This is not a new message! Indahl first discussed this in the non injury model way back in the 90’s Non-threatening explanation about back pain including movement helps repair & mobilise “worst thing to do is be careful” This a great message
https://journals.lww.com/spinejournal/Abstract/1998/12010/Five_Year_Follow_Up_Study_of_a_Controlled_Clinical.18.aspx
Lot’s of contributing factors We can see that there are many contributing factors across multiple domains that should be considered as well as tissue based factors Maybe the psychosocial fans the flames?
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)30480-X/fulltext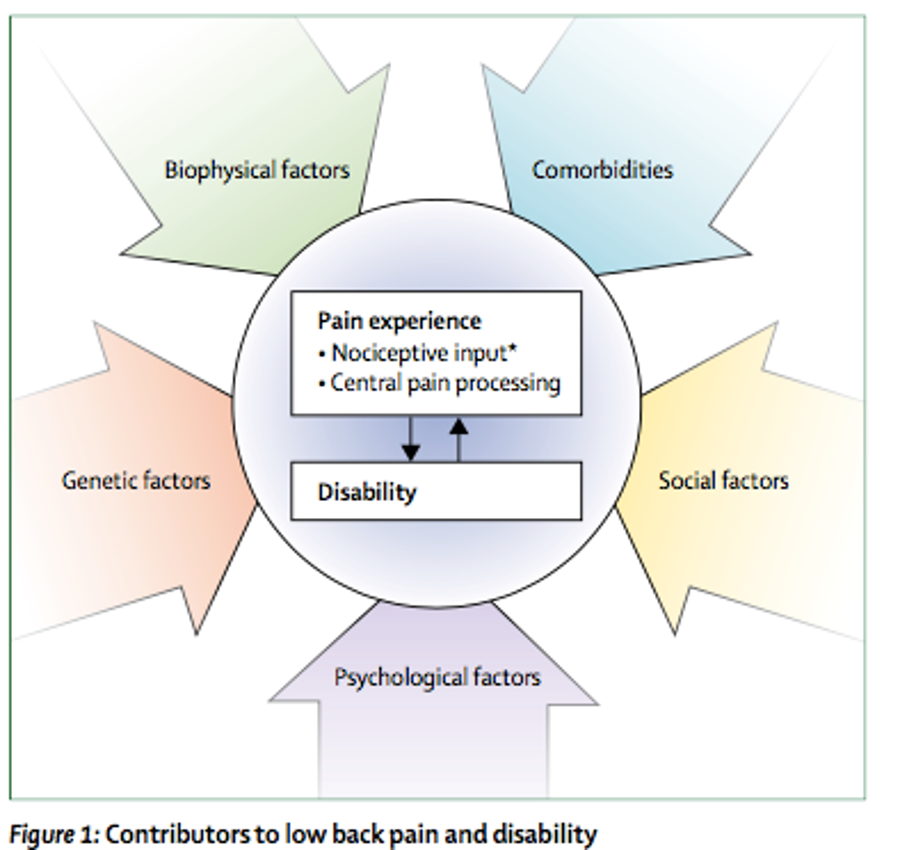
No really, Its complex… This diagram helps us to visualise how many things have been researched into relation to back pain Often clinicians & patients are looking for one singular factor that explains everything
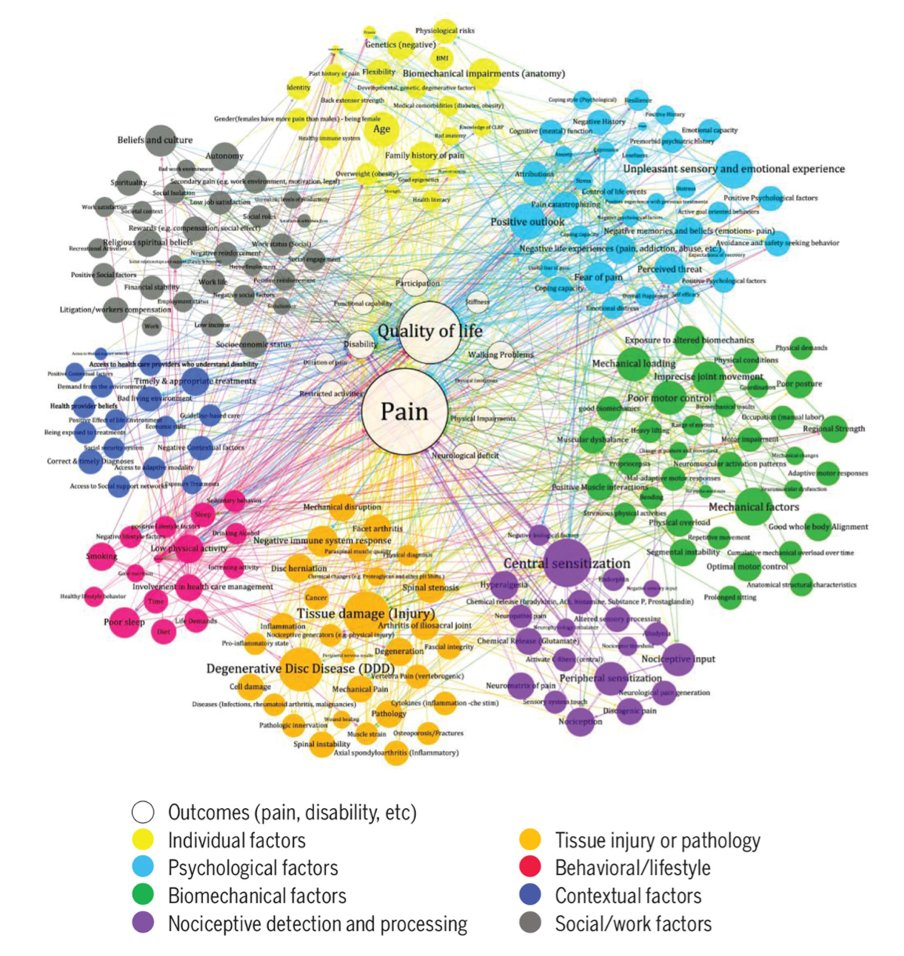
It’s still seen as biomechanical “The participants’ emphasis on biomechanical factors, was more than double that of psychological factors & more than five times placed on social factors, strongly contrasts with contemporary recognition of LBP as BPS”
https://pubmed.ncbi.nlm.nih.gov/35045354/
What’s the timeline/prognosis? NICE suggest it lasts on average between 2 & 6 weeks This is backed up by RCT data such as the FREE Back trial where 88% of the cohort, broad inclusion criteria, had significant recovery inWhat’s the timeline/prognosis
https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1002897

Prognostic factors Prognostic factors effect outcomes over the longer term, here are some of common factors that have been identified
baseline pain
duration of symptoms
pain self efficacy
Passive coping score
Low predictions of recovery
ncbi.nlm.nih.gov/pmc/articles/P
This is why it can be reoccurring condition! Chronic NSLBP often can be fluctuating & episodic. “LBP is often an episodic condition. This episodic nature also means that the course of LBP is not well described by an overall population mean”
musculoskeletdisord.biomedcentral.com/articles/10.11

Clinical care
This is suggested as a clinical care overview from the initial appointment to follow up and also potential referrals
https://www.safetyandquality.gov.au/standards/clinical-care-standards/low-back-pain-clinical-care-standard

